Epi Weekly: Worse and Worse, Every Week
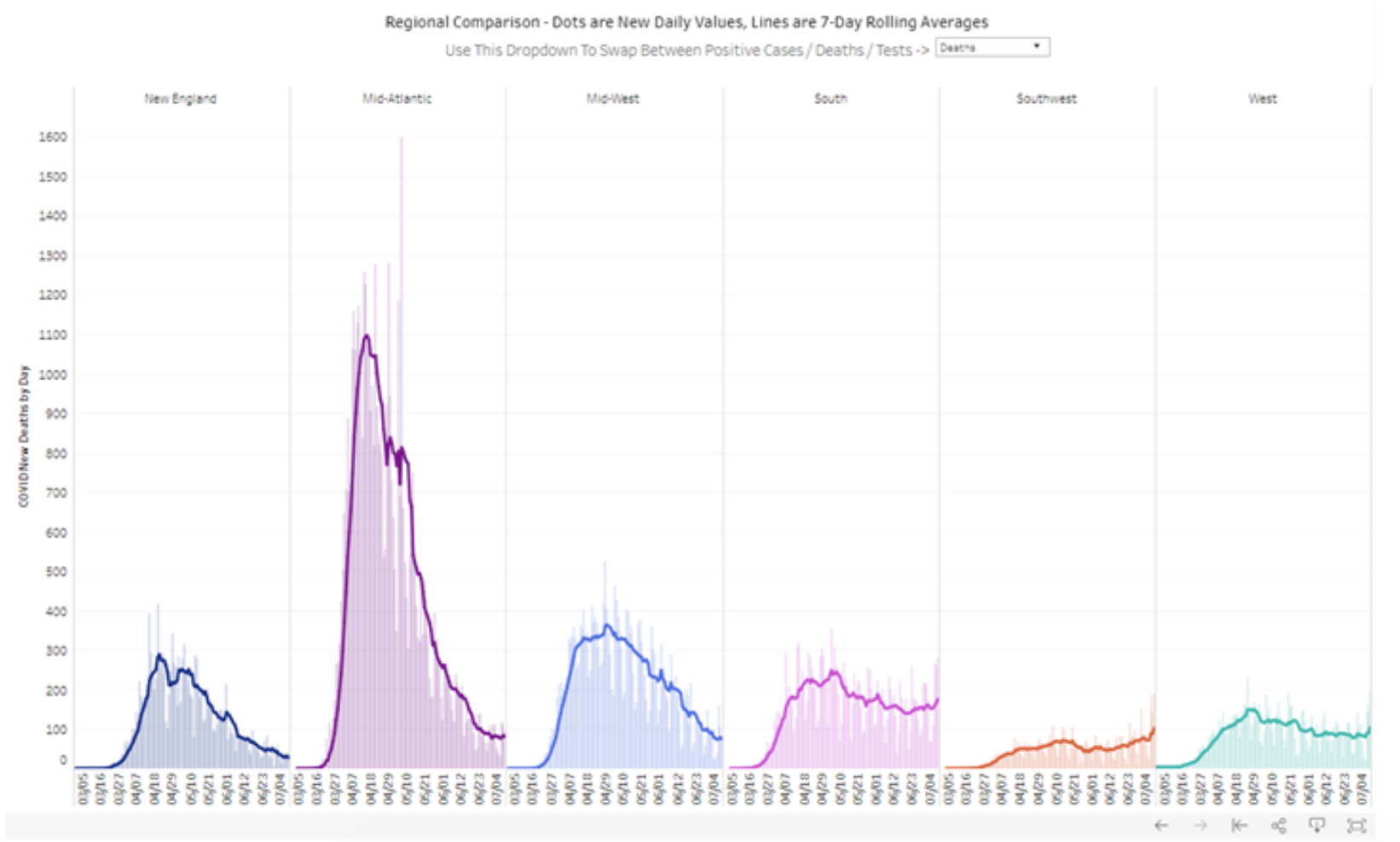
Cases are increasing exponentially in most of the US. The current epicenter is the Midwest. Diagnosed cases have been in the 150,000–200,000 range, but there are likely at least half a million new infections each day. In South and North Dakota, an estimated 1 in 11 people have Covid. This figure from the Covid Tracking Project shows key trends.
As per CDC’s CovidView weekly, test positivity, which remains one of the most important indicators of disease spread, increased from 10.8% to 11.9%. One of the analysts I follow closely is @youyanggu, who just launched a nowcasting site. He estimates that there are 3.3 infections for each diagnosed infection. In other words, the case detection rate (CDR) — the proportion of all infections diagnosed — in approximately 30%. The CDR is difficult to estimate, but it is very important, and I’ll return to this topic in the future article.
Although not all people who are estimated to have illness are infectious (maximum infectivity starts about 2 days before and continues for about 5–7 days into illness), nationally approximately 1 in 100 people, and possibly more, are infectious today. The analysis and map by Youyang Gu https://covid19-projections.com gives estimates.
The US has the highest rate of hospitalizations from Covid ever. Deaths are increasing. Further increases inevitable — but continued increases are not (more on this later). Excellent graphic from the folks at Covid Tracking Project. Midwest is having a crescendo. Cases in the Northeast are increasing. In the South, cases never decreased much, and now are increasing. Cases in the West are increasing https://bit.ly/3kQONPy
Hospitalizations are increasing steadily. Already many are stretched; it’s likely we’ll see another 30,000+ increase in coming weeks, increasing from 70,000 to 100,000. The scarcest resource: trained healthcare staff. PPE remains insufficient. Nursing home cases are increasing. And all of this will get worse. 4/10
If our plans don’t change, Thanksgiving will be the Super Bowl of super spreader events, accelerating an epidemic already out of control. Good guidance from CDC. Better a Zoom Thanksgiving than an ICU Christmas. Read my latest op ed about where we are and what we can do for the holidays. At Resolve, we created the graphic below — important to understand that degrees of separation and connection are much broader than we realize.
In President Obama’s book, he writes:
“The pandemic we’re currently living through is both a manifestation of and a mere interruption in the relentless march toward an interconnected world.”
There’s continued and very encouraging news on vaccines. But there are still many unknowns. It remains to be seen how rapidly supply will increase, how long immunity will last, whether there will be strong protection of frail elderly people such as many who are in nursing homes, and whether there will be rare safety problems identified when millions of people are vaccinated. And as distribution begins, it will need to be fast, fair, and transparent. Nursing home staff and residents should get first, and it’s encouraging that the current administration seems to be planning for this. It’s crucial that there be a smooth handoff to the incoming Biden administration — this is going to be the most complicated vaccination program in the history of the United States. Good report by the Kaiser Family Foundation, with some key findings below. States have made some progress but much more is needed, and states need money to prepare and implement. Congress must act.
A vaccine won’t be widely available for many months — so we need to have much better control for many more months. The New York Times has a GREAT graphic presentation showing that policy matters.
Here’s a sad tale of 2 states. Vermont is 6 times more densely populated than South Dakota, but has 16 times fewer cases and 10 times fewer deaths. Following science saves lives. I outlined how we can make progress using a one-two punch strategy with more nuanced closures and more effective testing and isolation.
Hong Kong and Singapore created a travel bubble. If there are more than 5 unlinked infections per day, they will stop travel. Yesterday there were approximately 500,000 unlinked infections in the US — an astounding 100,000 times more. With a new approach based on science, organized response, and honest communication, together we can make steady progress.
Masks and mask mandates work! Important report from CDC. Impressive graphics — the line graph is worth careful study. Freedom includes freedom from disease. That should not be hard to understand.
I wish you all a happy, socially connected, physically distanced Thanksgiving!
“Wear gratitude like a cloak and it will feed every corner of your life.
― Rumi
Covid Epi Weekly: Death Won’t Take a Holiday this Holiday Season
(Article initially published on Tom Frieden’s LinkedIn: https://www.linkedin.com/pulse/covid-epi-weekly-death-wont-take-holiday-season-tom-frieden/)
We have a divided government and a divided country, just when we most need unity to stop the pandemic. Covid is skyrocketing across the country, but some areas are being hit much harder than others. Correcting for how much testing is done, there’s a 100-fold difference between South Dakota and Vermont and 10-fold difference between the Northeast and Upper Midwest.
How bad is the increase we’re seeing? Bad. Cases are doubling, tripling, or more in many communities and states. Much of the US is in the exponential increase phase, and every day of delay costs lives. The basic 1-2 punch concept still applies. 1) Knock the virus down, minimizing societal harm, and 2) Keep it down.
First, let’s take a look at the numbers. They’re bad almost everywhere. According to the CDC, national percent positivity increased (from 7.2 to 8.2%), and increased among all age groups in all regions. Horrifying. This is a national tsunami. Hospitalizations are up 14% and deaths up 8%. Deaths follow hospitalizations by a week or two. These numbers will continue to rise.

Many thanks to Covid Exit Strategy for their great work tracking the situation in each state. I hope the site, and others, like it, will be put out of business by a competent federal response that gets us all on the same page and demonstrates that our only enemy is a virus. The more we work together, the more we can control Covid.

The increases in hospitalizations required the Covid Exit Strategy team to add a new color. The Upper Midwest is in the exponential increase phase. Here’s the key point: the per capita hospitalization rates for Covid range from 500 per million to <50/million. That’s a 10-fold difference. Policy matters! Covid can be controlled.

It’s been frustrating to see a continued focus on the wrong numbers. Detected cases are only about one fifth of total infections. A weighted ranking of test-intensity and incidence helps. As I mentioned at the beginning of this post, there’s a 100-fold difference between South Dakota and Vermont.

We’re waking up to the fact that we need to shut down. We can do this sensibly, keeping schools, childcare, universities, shopping, barber shops, and other places open—but ONLY with rigorous safety measures and modifications. We will need to reduce travel and risky indoor gatherings. Ireland’s approach is a great example.

Like oh-so-much-too-much in our society, Covid hurts the most vulnerable most. Rates of infection are vastly higher in Native American, Latinx, and Black communities. The virus doesn’t stay in any group—we’re all connected. The more safe we all are, the more safe we all will be.

Sooner or later, we’ll have to knock down the spread of the virus with strategic closures. But we need to vastly up our game in preventing household spread.
A stunning study found a very high attack rate among children in families with Covid: 77%!

Other studies have found lower rates, but the bottom line is not finding people who are infected fast and helping Covid patients relocate during maximum infectivity extends explosive spread by weeks or months. We must reduce the time from infectivity to isolation, offer paid sick leave for all, and make isolation more effective. Knocking down spread is the first punch, boxing the virus in when new infections emerge is the second punch.
We must discover more, such as how to avoid leaving infectious people at home, how to best use the tens of millions of antigen tests being sent out, and how to scale production of N95 (including safely reusable) and surgical masks.
Pandemic fatigue is understandable. We all feel it. The WHO Euro released a helpful report showing how we can help address it:
● Understand and empathize
● Engage communities to find solutions
● Reduce restrictions but protect lives
● Be transparent, consistent, predictable, and fair.
The virus isn’t giving up, and neither can we. Success is possible. It takes rigor, discipline, patience, and working together. This CDC article shows the positive impact of targeted closures and widespread use of masks.

The sooner we shut, the softer and shorter we can shut. We can minimize disruption to holiday shopping, jobs, education AND reduce major drivers of spread. To have happier holidays, we need to stay much safer for the next six weeks.
Covid Epi Weekly: Harrowing Holidays
(Article initially published on Tom Frieden’s LinkedIn: https://www.linkedin.com/pulse/covid-epi-weekly-harrowing-holidays-tom-frieden/)
It’s hard to imagine a worse confluence. Cases are surging in much of the US. People are tired of the limitations the virus is imposing. Economic harm is real, painful, and persistent. And White House communications have continued to mislead, divide, and deny.
Bottom line (almost) up front: there IS one thing that can stop Covid. For months I’ve said there isn’t one thing, but there is. Not masks. Not travel limitations. Not staying home. Not testing. Not contact tracing. Not isolation. Not quarantine. Not even a vaccine.
It’s TRUST.
Around the world, the best predictor of controlling Covid is social cohesion: the understanding that we’re all in this together. We’re all safer when we all mask up, stay home when we’re sick, support contact tracing, and, eventually, get vaccinated. No group can get the infection without endangering other individuals and groups.
That’s why the unspoken advocacy for herd immunity by this White House is so revealing. “Protect the vulnerable” sounds great. But doing that while allowing the virus to spread among the young is an impossibility. It’s a scientific blunder emanating from a philosophical error.
When we understand we’re all connected, we can win. Let’s prioritize getting services to people and communities most in need. Let’s protect ourselves, our families, our community. There’s only one enemy: a virus. White House divisiveness is the best ally the novel coronavirus could possibly have.
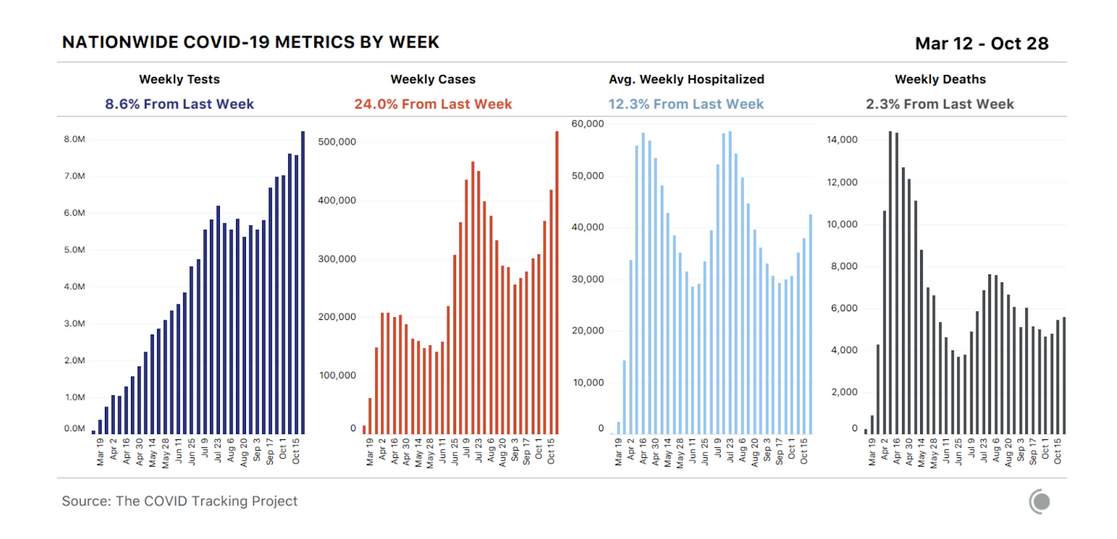
Now, the disheartening numbers. Detected cases are up three times more than testing. Testing is up 8.6%, while cases are up 24%. What’s more, test positivity has risen from 6.6% to 7.1%. Saying cases are up because of more testing is like saying gravity isn’t real. This is an informative, though depressing graphic from The Covid Tracking Project.
Here’s a good way to show that cases are increasing much faster than testing by state. Case growth has been much higher than test increases in all states. (The published data from Mississippi has been whipsawing.)

Reported cases fluctuate by day. Generally, see lower case numbers over the weekend because of fewer office visits and tests. The weekends are time off for many people, but not for the virus. Paying attention to the seven-day average of reported cases is more useful.
Hospitalizations are, of course, increasing following case increases. It’s shameful and inexcusable that the federal government is not publishing data it has on the pandemic. NPR obtained a recent daily report from the US Department of Health and Human Services, and here’s a screenshot showing hospitalizations increasing:

Will deaths increase? Does night follow day? Of course. We ardently hope that deaths won’t increase as much as in the past, due to better care, fewer overwhelmed hospitals, and the use of dexamethasone and possibly other treatments. But only time will tell. Deaths follow case increases by about three weeks.

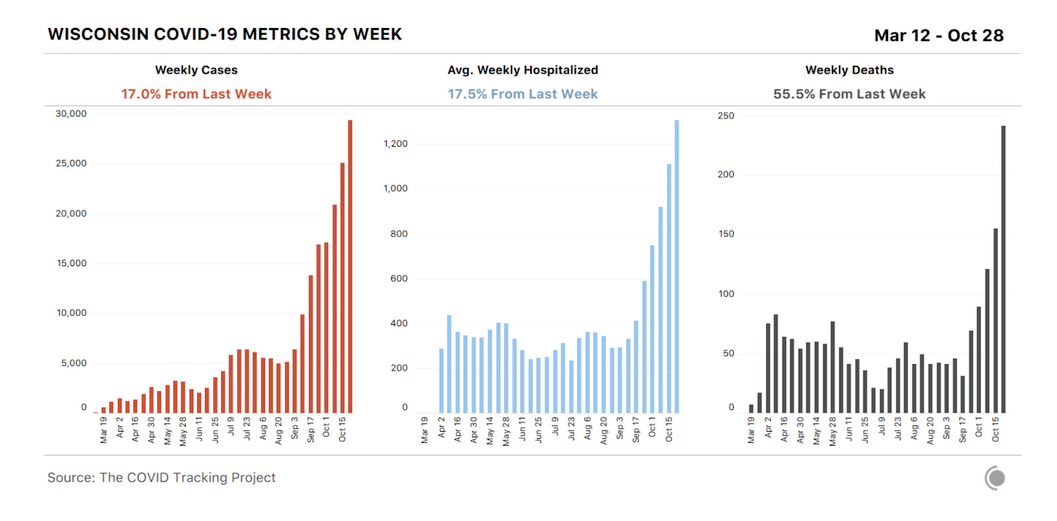
Wisconsin is a bellwether … including for Covid deaths. The state has seen a huge increase in Covid deaths. Many other states, sadly, aren’t far behind.
As an epidemiologist, I think a lot about numbers. This week, two numbers made a big impact on me: 13 and 9.
● 13 is the number of years of life lost on average for each of the 230,000+ Americans killed by Covid.
● 9 is the number of people, on average, grieving for each of those deaths.
These represent millions of tragedies, most of the preventable.
We public health specialists must never underestimate the health and social impact of economic harm. We’re heading into a dark winter. We can limit harm with more outdoor activities, open schools, social connections, and shopping. And by reducing indoor maskless contact in poorly ventilated spaces.
I’ve shared some bad news so far. Here’s some good news. 9 of 10 people understand the importance of masking up. Those who don’t are a small, misguided minority. Masking up correlates well with lower case counts. Mask mandates, if done well, boost mask use and save lives.
The increase in telemedicine is also good news. Primary care is the most important part of our health care system, but it’s also the most underfunded and neglected. If we get regulation and reimbursement right, telemedicine will be an important part of fixing primary care and our health care system.
An interesting data survey summarized by Covid Exit Strategy shows that in states with more than 90% mask wearing, less than 20% of people know someone who is sick. In states with 80% or less mask wearing, 30-54% know someone who is sick. Look at the top and bottom places here—the gap is striking!

One of the many, many failures of this administration’s response to Covid has been insufficient protective equipment for health care workers. It makes me SO ANGRY. We’re sending our troops into battle without the armor a competent government would have provided.
Case increases lead to a vicious cycle: longer test turnaround, overwhelmed public health, less isolation of infected patients, more cases. If we reduce cases by wearing masks, watching our distance, washing our hands, and avoiding risky indoor spaces, we can create a virtuous cycle: fewer cases, better contact tracing, and enhanced ability to stop spread.
Why harrowing holidays? Thanksgiving in Canada. The country has struggled with case increases, division, attempts to undermine science, and denials of reality. Even countries which have done relatively well are now struggling. The US, with a completely failed federal response, faces potential devastation.
“Ending the COVID-19 pandemic”? The claim in this White House letter is Orwellian.

The reality is the pandemic won’t end anytime soon. But maybe, soon, there will be an end to the completely dysfunctional national response.
Covid Epi Weekly: Turning the Corner on Covid in the US—Into an Oncoming Tsunami of Cases, Hospitalizations, and Death
October 23, 2020. You know what’s NOT tired of winning? Covid. Covid’s not tired of winning. Unless we up our game, Covid will keep winning, keep spreading, keep killing Americans—preventably.
Test positivity is increasing in ALL age groups. Positivity in people over the age of 65 increased from 3.6% five weeks ago to 5.2%—a 44% increase. Five weeks ago, the rate in young adults was 50% higher than in those over 65; last week the rate was just 20% higher. This confirms that what started in the young didn’t stay in the young.
Cumulative hospitalizations for adults over 65 in the US:
1 in 300 White people
1 in 120 Native American people
1 in 110 Latinx people
1 in 87 (!) Black people.

The emergence of Covid has exacerbated racial injustice in health. Black and Latinx communities already had less access to health care. The inadequate protection of essential workers, many of whom are Black/Latinx, has also magnified inequities.
Years of life lost is a good way to measure the burden of a public health crisis, though it’s far from perfect. There have already been 2.5 million life years lost, more than 13 years for every one of the 225,000 people who have died from Covid. Think of the joy, happiness, and meaning lost for each of those 13 years. Each of those 2.5 million years.
A working paper published in June by former NYC Health Commissioner Dr. Mary T. Bassett showed the same pattern: Black and Latinx people in the US make up 33% of adults but 74% of early death. This is horrifying. Valid responses to this information include rage and action.
Other than Northeast, this map is bleak.

Although it’s clear that there is a worsening situation in the US, we’re flying blind as to exactly how and where Covid is spreading. Test positivity is less informative than it was before. Case rates are an even worse indicator. The record 85,000 infections reported for Friday represent only about 20% of all infections. The failure of federal leadership means we’re not tracking the right indicators.
Take a look at the Dakotas. Neither state has a mask mandate. They are losing to Covid. The reported rates are slightly higher in North Dakota (1,000 vs. 800 per million a day), but when corrected for test intensity, South Dakota has about 4x the rate of North Dakota and 20x the rate of the Northeast. In other words, South Dakota looks not as bad, but it’s actually much worse.



Increasing cases in Alaska suggest that colder weather may favor the virus. In the classic Art of War, Sun Tzu defined five factors that determine success or failure in war: moral influence, weather, terrain, leadership, and strategy. In our war against Covid, the US is not organized for success in any of those 5 - we’re zero for 5 at present.
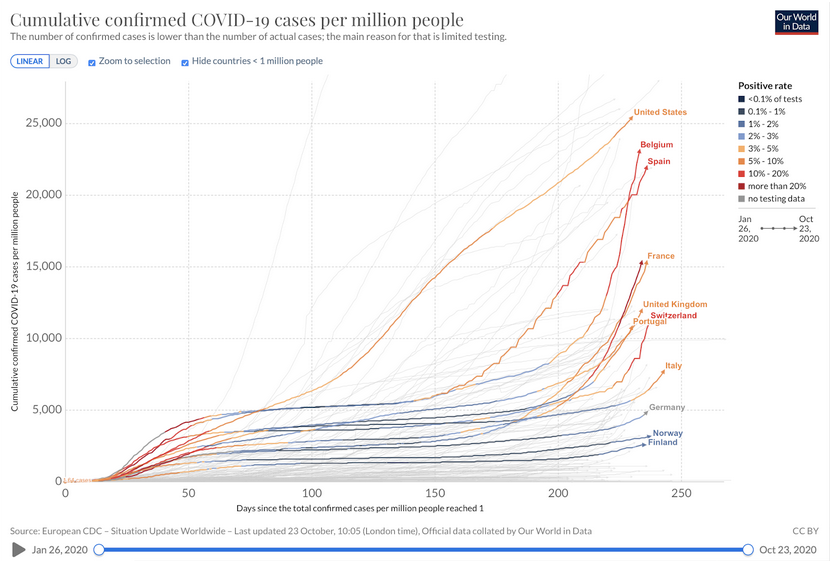
Parts of Europe are also getting hit hard. Places that didn’t drive cases down enough to find and stop clusters face the ever-present risk of explosive spread. Some countries didn’t flatten the curve sufficiently (Spain, France, Italy, UK, Belgium) and some did (Germany, Norway, Finland).


Economic pain is real, and deadly. We are all impatient to resume activities we miss, but the reality is there are things we won’t be able to do until we control the pandemic. Here’s more evidence the virus, rather than control efforts, is what’s suppressing economic recovery. “It has almost nothing to do with regulations.” Paraphrasing James Carville, to fix the economy, it’s the pandemic, stupid.
Balance is key in our response. We must apply more granularity to our “circuit breakers” to stop Covid. Yes, we’ll have to adapt our lives for the foreseeable future. But there are a lot of activities we can and should do, while taking steps to reduce risk. Schools, healthcare, workplaces, stores can open more safely. Spending time outdoors is great. On the other hand, travel from places with high Covid to places with low Covid is a recipe for spread. Restaurants, bars, and indoor get-togethers amplify the virus and we’ll need to figure out how to do this as safely as possible.
The higher the peak, the longer it lasts. The lower Covid goes, the longer it takes to come back. As we sow, so shall we reap. Hyperbolic discounting is not in our favor here. As night follows day, hospitalizations and deaths follow cases, which follow letting our guard down.
Civic responsibilities include not harming (e.g., infecting with coronavirus) others, staying informed, paying taxes, participating in your community. And VOTING. We released materials on voting more safely. I like the message below. Please spread the word.

Covid Epi Weekly: Harrowing Holidays
It’s hard to imagine a worse confluence. Cases are surging in much of the US. People are tired of the limitations the virus is imposing. Economic harm is real, painful, and persistent. And White House communications have continued to mislead, divide, and deny.
Bottom line (almost) up front: there IS one thing that can stop Covid. For months I’ve said there isn’t one thing, but there is. Not masks. Not travel limitations. Not staying home. Not testing. Not contact tracing. Not isolation. Not quarantine. Not even a vaccine.
It’s TRUST.
Around the world, the best predictor of controlling Covid is social cohesion: the understanding that we’re all in this together. We’re all safer when we all mask up, stay home when we’re sick, support contact tracing, and, eventually, get vaccinated. No group can get the infection without endangering other individuals and groups.
That’s why the unspoken advocacy for herd immunity by this White House is so revealing. “Protect the vulnerable” sounds great. But doing that while allowing the virus to spread among the young is an impossibility. It’s a scientific blunder emanating from a philosophical error.
When we understand we’re all connected, we can win. Let’s prioritize getting services to people and communities most in need. Let’s protect ourselves, our families, our community. There’s only one enemy: a virus. White House divisiveness is the best ally the novel coronavirus could possibly have.
Now, the disheartening numbers. Detected cases are up three times more than testing. Testing is up 8.6%, while cases are up 24%. What’s more, test positivity has risen from 6.6% to 7.1%. Saying cases are up because of more testing is like saying gravity isn’t real. This is an informative, though depressing graphic from The Covid Tracking Project.
Here’s a good way to show that cases are increasing much faster than testing by state. Case growth has been much higher than test increases in all states. (The published data from Mississippi has been whipsawing.)
Reported cases fluctuate by day. Generally, see lower case numbers over the weekend because of fewer office visits and tests. The weekends are time off for many people, but not for the virus. Paying attention to the seven-day average of reported cases is more useful.
Hospitalizations are, of course, increasing following case increases. It’s shameful and inexcusable that the federal government is not publishing data it has on the pandemic. NPR obtained a recent daily report from the US Department of Health and Human Services, and here’s a screenshot showing hospitalizations increasing:
Will deaths increase? Does night follow day? Of course. We ardently hope that deaths won’t increase as much as in the past, due to better care, fewer overwhelmed hospitals, and the use of dexamethasone and possibly other treatments. But only time will tell. Deaths follow case increases by about three weeks.
Wisconsin is a bellwether … including for Covid deaths. The state has seen a huge increase in Covid deaths. Many other states, sadly, aren’t far behind.
As an epidemiologist, I think a lot about numbers. This week, two numbers made a big impact on me: 13 and 9.
● 13 is the number of years of life lost on average for each of the 230,000+ Americans killed by Covid.
● 9 is the number of people, on average, grieving for each of those deaths.
These represent millions of tragedies, most of the preventable.
We public health specialists must never underestimate the health and social impact of economic harm. We’re heading into a dark winter. We can limit harm with more outdoor activities, open schools, social connections, and shopping. And by reducing indoor maskless contact in poorly ventilated spaces.
I’ve shared some bad news so far. Here’s some good news. 9 of 10 people understand the importance of masking up. Those who don’t are a small, misguided minority. Masking up correlates well with lower case counts. Mask mandates, if done well, boost mask use and save lives.
The increase in telemedicine is also good news. Primary care is the most important part of our health care system, but it’s also the most underfunded and neglected. If we get regulation and reimbursement right, telemedicine will be an important part of fixing primary care and our health care system.
An interesting data survey summarized by Covid Exit Strategy shows that in states with more than 90% mask wearing, less than 20% of people know someone who is sick. In states with 80% or less mask wearing, 30-54% know someone who is sick. Look at the top and bottom places here—the gap is striking!
One of the many, many failures of this administration’s response to Covid has been insufficient protective equipment for health care workers. It makes me SO ANGRY. We’re sending our troops into battle without the armor a competent government would have provided.
Case increases lead to a vicious cycle: longer test turnaround, overwhelmed public health, less isolation of infected patients, more cases. If we reduce cases by wearing masks, watching our distance, washing our hands, and avoiding risky indoor spaces, we can create a virtuous cycle: fewer cases, better contact tracing, and enhanced ability to stop spread.
Why harrowing holidays? Thanksgiving in Canada. The country has struggled with case increases, division, attempts to undermine science, and denials of reality. Even countries which have done relatively well are now struggling. The US, with a completely failed federal response, faces potential devastation.
“Ending the COVID-19 pandemic”? The claim in this White House letter is Orwellian.
The reality is the pandemic won’t end anytime soon. But maybe, soon, there will be an end to the completely dysfunctional national response.
Covid Epi Weekly: Immunizing Against Herd Stupidity
It’s been a bad week in the fight against Covid. We’ve seen reopenings without sufficient care. Failure by infected people to isolate. Failure to communicate consistently, effectively, respectfully, empathically. A dangerously misguided theory on immunity. Throughout the country, cases are increasing. This will inevitably be followed by increased hospitalizations, and then by increasing death rates.
Test positivity increased for the first time in a month (to 5.4%), but positivity is now more difficult to interpret due to new antigen tests and a lack of consistent definitions and reporting. Hospitalization data is concerning, though in the crazy world of US health economics supply creates demand.
In the past two weeks, 21 states reported their highest Covid rates ever, including in most of the Midwest and much of the West. As predicted, we’ve surpassed 50,000 reported cases per day. The White House cluster is up to 40 known cases and hundreds remain untested. Only two states—Maine and Vermont—are still encouraging.
More information on long-haulers is emerging. We must better understand and care for people who are suffering from the persistent effects of Covid for months after their infection. This excellent article by the incomparable Jane Brody lays out what we know and what we’re trying to find out.
Some people have shamefully misrepresented a recent CDC study which found restaurants, bars, and close contact with Covid patients associated with illness. It’s infuriating to see this kind of misrepresentation, and it’s on par with Wakefield’s fraud on vaccines.
Here’s some great new data on self-reported mask-wearing. More masks → less illness. Masks are a low-cost, effective way to reduce spread.
No place where more than 90% of people said they regularly wear masks had more than 20% of people say they know someone who’s sick. On the other hand, no place where less than 85% of people said they regularly wear masks had less than 20% say they know someone who’s sick. How in the world did masks become political? They’re only against a virus, not a party or person. There’s only one enemy here, and that enemy is the virus that causes Covid.
Three pieces of bad news from this past week:
Remdesivir doesn’t appear to reduce death.
The US continues to fail at contact and source case tracing. This is complex, important, high-skill, high-empathy work.
The dangerously misguided concept of herd immunity through natural infection is spreading.
The reality is that we’re all connected. Infections in healthy people lead to infections in others. “Protecting the vulnerable” requires reducing the risk of infection in everyone. Although the more people who are immune, the slower virus spreads, every infection is a setback, not a step forward. This is not a complicated idea: The way to protect the vulnerable is to have fewer infections, not more infections.
Now three pieces of good news:
At least 199 out of 200 people with the infection recover. Covid is NOT the zombie apocalypse.
Dexamethasone and other steroids—cheap, available meds—reduce the likelihood of death by as much as a third.
Lots of safer social and economic activity is possible.
With Halloween and Thanksgiving coming, we CAN have some safer connections. I shared some ideas on how Halloween can happen without increasing the spread of Covid. For Thanksgiving, I’d suggest that all family members adhere to a strict two week quarantine before any get-together, and only plan to gather if travel can be done safely. That’s what my family is doing.
Let’s not get ahead of ourselves on vaccines. They are our best tool, but just one of many. We don’t know if they will be effective, safe, accessible, trusted. We don’t know how well they will work, how safe they will be, and for how long they will protect people. And even if they are safe, effective, accessible, and trusted, they won’t end the pandemic, and rare, serious adverse reactions may occur. Even if only 1 in a million people, or 1 in 100,000 people have a bad reaction, that’s a lot of people for a vaccine which billions of people may take. It’s always better to underpromise and overdeliver.
Simple measures such as ensuring paid sick leave are also very important. An interesting new analysis found that there was “roughly 1 prevented COVID-19 case per day per 1300 workers who newly gained the option to take up to two weeks of paid sick leave.” This is so important, and would have so many benefits. Should be high on the priority list of all governments.
We in public health must do better understanding and empathizing with the social and economic pain of the pandemic. In the US, there are at least 30 times more people who have lost their job because of the pandemic than have lost their life.
But it’s important to remember, as Ghana President Nana Akufo-Addo said, “We know how to bring the economy back to life. What we do not know is how to bring people back to life.”
Covid is here to stay. We must live fully now, taking steps to protect ourselves and our loved ones.
“The present moment is the only moment available to us, and it is the door to all other moments.” -Thich Nhat Hanh
The First Cluster - Epi Weekly Update October 12
The cluster at White House is a symptom and a symbol of the federal government’s failed Covid response. From overconfidence in testing, to lack of basic safety precautions in crowded indoor places, to delayed isolation, incomplete contact tracing, and failure to quarantine, there have been so many preventable missteps.
If there’s one major lesson from this particular failure, it’s that testing doesn’t replace safety measures—testing is only useful as part of a comprehensive strategy. There are often false negatives, and even if a result is accurately negative in the morning, someone could still be highly infectious hours later. That’s why it’s important to reduce risky indoor gatherings and to follow the 3 W’s: wear a mask, watch your distance, wash your hands.
Masks are particularly important. It’s worth reading this edition of our Weekly Science Review by the wonderful Dr. Cyrus Shahpar. I learned from it and was surprised by how suggestive the evidence is. In addition to protecting others and yourself, masks may reduce inoculum and make it more likely that, if you do get infected, you won’t get severely ill.
Rapid isolation reduces secondary cases. There’s strong evidence that paid sick leave reduces the risk that people will work while infectious from the flu, and that is almost certainly the same with Covid. The only valid reason to leave isolation is for a medically necessary procedure.
Contact tracing needs to be done quickly and expertly to find all those who have been exposed to the virus, trace the source of the infection, expand the circle of those warned, and stop the outbreak. Let’s rebrand contact tracing and call it what it is: supporting people who got Covid and who were exposed to it. Instead of “case investigator,” why not “patient support specialist”? And instead of “contact tracer,” how about Covid prevention specialist?
Quarantine means not exposing others after you’ve been exposed. Testing negative is not a get-out-of-quarantine-free card—you can be infectious soon after a negative test. But we should be able to optimize quarantine conditions (a walk outside not near others?) and duration (some places exploring shorter quarantines, with rigorous safety measures after 8 or 10 days) based on data.
Here’s the epi curve of the White House outbreak from what has been publicly reported so far. The pattern strongly suggests common exposure on September 26 or 27. An investigation should be able to determine the likely source and identify those most at risk. And of course it’s possible to identify the source of the outbreak—it just requires wanting to and having the expertise.
The White House cluster isn’t over. There are likely to be other cases. Check out this great graphic from Cleveland Clinic. We need a series of measures to reduce risk, prevent illness and death, and accelerate economic recovery. I’ve been calling it a “comprehensive approach,” but does anyone have a better term?
Controlling Covid requires a one-two punch. In addition to practicing safety measures such as reducing indoor gatherings and the 3Ws, we have to do better boxing the virus in after a new case is identified. We do this through rapid isolation, complete contact tracing, and supportive quarantine. That’s the way we prevent cases from becoming clusters and clusters from becoming outbreaks.
In the US, hospitalizations and deaths are slowly trending downward, but that won’t last because cases are steady or increasing in most of the country. Only Maine and Vermont are reassuring. Unfortunately, there will be continued increases in cases, and eventually deaths. There will be 230,000 reported deaths by November 3. A sobering number. We have one of the highest cumulative death rates of all wealthy countries.
In New York City, we’re continuing to see uncontrolled spread in religious communities and increasing risk elsewhere. Note that this is the same community that had extensive spread in the spring - so hopes that a low level of infection will lead to herd immunity are false, and dangerous (more on this next week). The ONLY way to stop spread in this community is to engage the community, support and collaborate on education from within, and encourage religious leaders to establish and manage acceptable isolation facilities.
Some good news is that schools, if run well, don’t appear to be major amplification points for the virus. At Resolve to Save Lives, we’ve been saying since March that we must keep in-person learning as available as possible, which means reducing spread in the community and adapting the school environment and policies.
As the late New York Senator Daniel Patrick Moynihan said, “You’re entitled to your own opinion, but not your own facts.” And to quote epidemiologist William Farr, “The death rate is a fact; anything beyond this is an inference.” The cumulative US death rate has now passed the UK, approaching Spain, highest of high-income countries. Read the graph, and weep.
We cannot become hardened to horror of continuing, preventable Covid deaths. Every life is precious. Who saves a life, saves a world.
40 Million Plus 1 ... and NYC on the Brink of a Precipice. October 5 weekly Epi Update.
Although there have been 7.4 million reported infections in the United States with the virus that causes Covid, estimates suggest that the number of actual infections is about 40 million, at least. The infection of President Trump is the most prominent, and one of the most telling.
My thoughts are with the President, First Lady, their family, and all others infected with and affected by Covid. The President’s infection is a reminder that Covid is an ongoing threat. No one is safe – not even heads of state – until everyone is safe.
Risk of severe illness and death increases steadily with age. A 74-year-old has approximately a 3% chance of death. Once it became clear that he had symptoms, the estimated risk increased to about 10%. If he had a clear indication for hospitalization (moving him to Walter Reed was clearly the responsible thing to do, whether or not he had an indication for hospitalization), the risk could be as high as 25%. The risk is even higher in males than females, and higher in people who are obese, and lower with good care. 85-90% of those infected in their 70’s will have no, mild, or minor illness. Of those with symptoms in this age group, 90% recover.
People who get prompt medical care, including oxygen, likely have better outcomes. Remdesivir may reduce the duration of illness. The data on convalescent plasma is contradictory. Monoclonal antibodies, which the president received, are promising (especially early in illness) but unproven. Dexamethasone, which the president also received, may reduce the risk of death by about a third, but is generally thought to be most helpful late in the course of illness, when a patient’s own immune system, rather than the virus, is causing much of the harm.
Testing is only useful as part of a comprehensive strategy. What’s important isn’t how many people are tested or how often, but what is done with testing to reduce risk. Testing doesn’t replace wearing a mask, watching your distance from other people, and washing your hands.
It’s a plain truth that face masks protect others, and almost certainly protect yourself as well. The more people who wear masks when we’re near others, the safer we’ll all be. Did the extensive testing done at the White House give a false sense of security? Absolutely.
We need to rebrand contact tracing. Let’s call it what it is: supporting people who have Covid and those who were exposed to it. Could Vice President Biden and Chris Wallace be at some risk from the debate? Maybe. The louder someone talks, the greater chance the virus will spread.
Every person infected with Covid is a step backwards in our effort to slow the pandemic and reopen society. We’re nowhere near herd immunity, and getting there without a vaccine would cost hundreds of thousands of lives and millions of jobs.
We must better prevent and treat this virus. We’re all in this together, and the better we prevent and fight it, the more lives we can save, and the sooner and safer we can get to the new normal.
Overall in the US, most states had increases in Covid spread during the month of September.
The new trend feature on Covid Exit Strategy is helpful, although the trends are discouraging.
The only states with reassuringly low rates of Covid are Maine, Vermont, New Hampshire, and perhaps Connecticut. Many states, such as Florida, are opening despite persistently high positivity rates, and will inevitably have further increases in the coming weeks. These actions raise the question: is this action, which will increase cases in a month, intentional or just neglect of science?
Closer to (my) home, NYC is on the edge of a precipice. We’re seeing extensive and ongoing spread in religious communities and likely beyond, meaning there’s a very high risk of a resurgence. Here are the positivity rates in hotspots, according to Governor Cuomo (Media statements from the city government have shockingly lacked basic information on the number of people tested and positive cases, as well as on trends).
For more than a month, NYC has had 300 or so diagnosed cases a day, but we still lack basic information about how the city is doing. We need to know:
What proportion previously identified as contacts and were in quarantine already?
For how many was the source identified?
Average time from symptom onset, or test taking, to isolation?
Are cases isolating? Contacts quarantining?
It’s challenging to work with a religious community that doesn’t trust the government. How about hiring 1,000 people from the community through acceptable intermediary organizations to fight Covid? The key is to start ASAP, standardize training and performance monitoring, and get community buy-in.
Gandhi’s birthday was Friday. I think about his call to empathy and to recognize that our enemy is hatred. We’re all connected. Unless we work together to fight Covid, the virus will continue to have the upper hand.
Covid This Week: The Virus Strikes Back
(Original article published on Tom Frieden’s LinkedIn account https://www.linkedin.com/pulse/covid-week-virus-strikes-back-tom-frieden/)
People are tired of fighting the virus, but the virus isn’t tired of infecting people. As parts of Europe and the US show, if you turn your back on Covid, it will come back to bite you. Cases are trending up again in many states, and are likely to hit 50,000 a day in the US in October.

Trends in positivity are hard to track, and getting even harder to track. Per the Covid Tracking Project, only 9 states currently followthe best practice of reporting antigen and PCR tests separately. States should also report the proportion of unduplicated people who tested positive, cross-referencing the two types of test.

What starts in the young doesn’t stay in the young. The MMWR reports that young adult infections were followed a week or two later by infections in people over 60. We’re all connected. The sooner we recognize that, the sooner we can move forward more safely.
These are some of the top Covid hotspots.
Universities
Meatpacking factories
Jails, prisons
Homeless shelters
Meatpacking factories are driving spread in many communities, with persistent failures in prevention, response, and transparency. It’s crucial that we take action to stop spread in hotspots.
Covid is spread by particles – some large, some small. It's a continuum, not a dichotomy. In crowded indoor spaces, Covid can spread widely, but it’s much less infectious than measles. Measles commonly spreads through air that can stay contaminated for hours -- for example, people in an emergency department can get infected hours after a patient with measles has left. This is likely much less common with Covid than with measles. Transmission depends on the index case, ventilation, whether people are wearing masks, what activities they’re doing (singing, shouting, etc.), and who is exposed.
Recent spread in Orthodox areas of NYC is concerning. Given crowding and alienation from government, spread within the community is a near-inevitability, but wider spread in NYC can be prevented if the city does much better at rapid isolation and effective contact tracing.
For eight months, the US government has ignored, sidelined, and undermined public health and scientific recommendations. They have taken the tools we have to fight Covid and broken them. Masks. Testing. Effective communication. Contact tracing. Strategic closures. Careful reopening. These are all things we should be doing better.
Operation Warp Speed, the effort to deliver a Covid vaccine, has gotten some things right. For example, they’re testing multiple vaccine candidates, manufacturing in parallel with studies, and providing good CDC guidance on vaccine preparation. But if vaccine studies are stopped early, we’ll lose essential information on effectiveness in the elderly and safety for all.
Vaccines are our most important tool in the fight against Covid. We can only hope the administration doesn’t break this tool as well by meddling with the science and the approval process. Errors by the administration have already cost lives and jobs. Politicizing vaccination would be the most dangerous and costly mistake yet.
Covid Epi Weekly: One Step Forward, One Step Back
(Blog initially published on Tom Frieden’s LinkedIn account: https://www.linkedin.com/pulse/covid-epi-weekly-one-step-forward-back-tom-frieden/)
We’re seeing decreases in Covid cases and test positivity rates in much of the country. That’s good news. But there’s also been less testing, less information about how the virus is spreading, and impending explosions with schools and universities reopening.
“A single death is a tragedy, a million deaths is a statistic.” My primary concern is that people may become desensitized to the sheer number of deaths caused by the pandemic. Close to 200,000 people have been killed in the U.S. That’s staggering.
The positivity rate decreased from 5.5 to 5.1% nationally, which is progress. But we’re losing the ability to track the virus—new antigen tests are difficult to track, there’s been less testing overall, and there’s still no reliable information on who is being tested. We should be getting better information each week, but we aren’t.
Most of the US is still failing to contain Covid. There are too many cases to test, trace, isolate. Even in places with fewer cases, there’s very little tracking of actual outcomes of testing and contact tracing. We need to know the average number of days someone is infectious before isolation and the percentage of cases arising from among quarantined contacts. Tens of thousands of lives and millions of jobs depend on this.

It’s outrageous that we STILL don’t have reliable information on cases, hospitalizations, and deaths by week by race and ethnicity. Every place should report these numbers weekly. The disproportionate impact on Latinx and Black communities unacceptably high and indefensibly invisible.
Avoidable cases and deaths are heartbreaking. Avoidable economic decline is grinding. James Carville famously said, “It’s the economy, stupid!” Well, to get the economy back, “It’s the pandemic, stupid”. Unless we control the virus, we can’t get our jobs back.

Deaths matter most. The US will hit 200,000 deaths and the world will hit 1 million reported deaths in the next few weeks. Germany has had less than one-fifth the US death rate, Canada less than half, and South Korea 80 times less. Tens of thousands didn’t need to die from Covid. We certainly don’t want to be #1 in death.

On 9/11, I reflected on deaths. My group is called Resolve to Save Lives for a reason. But we risk getting hardened to tragedy. Ed Yong wrote a superb article on this phenomenon and more in The Atlantic. More than 1,000 Americans a day have died recently from Covid. Even at “only” 500 deaths a day in the U.S. this would represent:
More than all injuries
1.5x all Alzheimer’s deaths
2.2x all diabetes deaths
3x all overdoses
4x all suicide deaths
9x all homicides
32x all HIV deaths
In fighting the pandemic, communication matters. If the goal is to prevent panic and save lives, there’s a proven way of doing it: 1. Be first. 2. Be right. 3. Be credible. 4. Be empathetic. 5. Give people practical things to do to protect themselves, their family, and their community. Is it possible for the US national response to have violated these principles more than it did?
We can control Covid, but to do so we must chip away at it. Close the riskiest places. Mask up. Box the virus in (test, isolate, trace, quarantine). Improve ventilation. Every little bit can help, as long as there are a lot of little bits to get R<1 and keep it there. Vaccination can help if it's safe, effective, accessible, and trusted. IF.
A Message to Young People from a Public Health Doctor
(Blog initially published on Tom Frieden’s LinkedIn account: https://www.linkedin.com/pulse/message-young-people-from-public-health-doctor-tom-frieden/)
Young people are facing a lot of stress and uncertainty right now. Schools in many places are closing almost as soon as they reopen. Sports, concerts, and large gatherings are a no-go. Recent college grads are entering a flagging economy.
I received a note the other day from an 18-year-old high school senior who's concerned and feels he may be getting depressed about the future. He asked when he'll be able to attend a sports game or concert again, when he'll be able to visit his grandparents, and if we'll ever get back to normal life. He asked, Will this be forever? Are we doomed?
Anyone who’s definitive about certain things about Covid simply doesn’t know enough about Covid. This is a new virus. It’s spent less than a year living with humans and we’re learning more every day. It's helpful to address what we know right now and with what level of certainty.
Here are a few things we know, and my best take on our level of certainty:
The virus can be deadly, particularly for older people, for some people with underlying health conditions, and, more rarely, for the unlucky people who get very sick or die even without underlying conditions. About this, we are 100% certain.
Wearing a mask protects people around you, particularly if you wear it correctly, and particularly in indoor environments. About this, we are also basically 100% certain. That doesn’t mean masks are 100% protective, it just means that wearing a mask reduces the risk to others.
Wearing a mask may protect you from getting infected, and may possibly protect you from becoming very ill if you do get infected. This is likely, but not certain, and depends in part on what kind of mask you wear and whether you put it on, wear it, and take it off correctly.
People who have gotten very sick from the virus appear to make antibodies, including neutralizing antibodies. This is 100% certain.
Antibodies, particularly neutralizing antibodies, may protect at least some people who have recovered for at least some time against getting infected with Covid again. We hope this is true, but it is not yet proven. Many of us (myself included) think it is the case, but how well these antibodies protect, and for how long—or even if they protect at all—isn’t known. I wrote about the perils and promise of immunity here.
A vaccine that is safe and effective may become available by early 2021. Many people hope this is the case, but we will only know when studies are done.
Now, what does all that mean for the question about whether this will be forever?
First, I would assume that for the next year (at least) masks are going to be important, particularly when indoors and when there are many people in a space that isn’t well ventilated.
Second, I would also assume that, even if we have a vaccine, we’re going to need to adapt our lives in certain ways for at least a few years. That’s because a vaccine isn’t likely to be perfect, nor are 100% of people likely to take it. That doesn’t mean we won’t be able to get much of our former lives back, but it does mean there are likely to be some differences. I shared why we have to accept a new normal and the possible hurdles and limitations of a vaccine. My mother is 91 years old and used to love to sing in chorus, but there’s no way she can go back to doing that any time soon.
So, will we be able to go to an indoor concert safely in 2021? We don’t know. Germany just did a fascinating experiment. They had an indoor concert with everyone wearing masks, but repeated it 3 times—with distancing, with some distancing, and without distancing. We may learn from that.
Will we be able to go to sporting events in 2021? Outside, definitely. Inside—same as the concert, we don’t know. (We do know that the louder people shout or sing, the more they can spread the virus, though much less so if they’re wearing a mask.)
Will we be able to go to indoor concerts and indoor sporting events safely in the next few years? I think yes. By then, we’ll almost certainly have a safe and effective vaccine, and we’ll certainly have better treatment. And I hope we’ll have a better public health system so that we can quickly test, trace, isolate, and quarantine so that when there are cases they don’t become clusters, and clusters don’t become outbreaks.
I don’t think masking will be forever, but I do think there will be some changes in how we go about our lives for the foreseeable future. Handshakes are probably out for a while. We should learn from Asia and wear a mask if we don’t feel well—or, better yet, stay home.
There’s actually an article about how to hug grandparents and other elderly loved ones more safely. And what my brothers and I do is to quarantine for 14 days before we see our mother, and maximize time outside together when we do see her.
We’re definitely not doomed. We—especially young and thoughtful people—have enormous potential to control our future. Even without a vaccine or treatment, communities in countries around the world have stopped the spread of the virus and gone back to life almost as before. With a vaccine and treatment, even more progress will be possible. Ironically, to get our individual freedom back, we need to work together.
The United States is Both Stalling and Failing in Our Effort to Combat Covid
(Blog initially published on Tom Frieden’s LinkedIn account https://www.linkedin.com/pulse/united-states-both-stalling-failing-our-effort-combat-tom-frieden/)
September 5, 2020. Continued spread of Covid in the US will continue to undermine health, jobs, economy, and education. A concerted, strategic approach would help, a lot. Parts of the Federal government are making a fundamental error: Failure to recognize we’re all connected, all in this together. Spread in any place or group is a risk everywhere, and if we work together, mask up, increase distance, improve testing, tracing, and support for patients and contacts, we can get more of our economy, more of our jobs, and more in-person education back.
Some are speaking about this outbreak as if it’s in the past tense. But more than 4 out of 5 Americans aren’t yet infected - it could get a lot worse, and it will if we don't improve our approach.
According to CDC’s CovidView, test positivity inched up from 5.4 to 5.5% in the past week, driven by an increase in positivity among 19-49-year-olds (and this is before many colleges try to open). Test positivity is at low levels in the northeast and some other states, but very few places are finding where most spread is occurring - most sources of infection, and even fewer -- maybe none -- are quarantining most contacts effectively. Because of that, virtually everywhere, the risk of explosive outbreaks remains. Rates of infection and of test positivity are high or increasing rates in most of the US. These rates are too high for economic and social recovery.

There are two data sources of note. County-specific test positivity, which should be open source but at least is available here (image below -- I wish they had zip code lookup).

And we’re delighted to work on the Covid Symptom Data Challenge. This could become an important early warning system for Covid. The competition is open until September 29.
Deaths and hospitalizations continue to decrease overall. But 500-1,000 deaths/day is horrific. These deaths also reflect approximately a quarter of a million infections per day a month ago (so we’ve only been detecting about 1 in 5 infections).
There were 215,000 more US deaths March-July than baseline. Of these, 71% were diagnosed as Covid by their doctor. The remainder were either undiagnosed Covid or deaths from Covid-disrupted care. Covid-disrupted care is an even greater risk in Africa and elsewhere, where measles, malaria, and other causes of death can rapidly and drastically increase death rates. Good tracker by The Economist.
Imagine how many fewer deaths the US could have had if the Federal government had focused right. One example: masks vs. hydroxychloroquine. Masks work. Places around the world that used masks consistently had half to two thirds less spread. 100,000+ deaths could quite possibly, simply, and cheaply have been prevented.
Good news on steroids. Confirmation that they help with severe Covid. The sicker you are, the more they help, with up to a 35% reduction in risk of death in the sickest patients. Yes, really, 35%. Nice review of all key data by WHO. Yes, really, WHO. Press conference, anyone?
I’m guardedly optimistic that we’ll have evidence of a safe and effective vaccine in the next few months. But we need to look at all the data. Efficacy is more likely to be proven early than safety. So when one CEO spoke recently of having early data because there are lots of events, that’s a big concern, because the events he’s talking about are Covid infections in trial participants who got placebo. We need transparency about what safety signals are being looked at. There are at least two important concerns about safety:
Inflammatory reactions. MIS-C in children - the Kawasaki-like syndrome - is the result of immune over-reaction. Will this happen with a small proportion of people vaccinated? How will we know? What sample size is needed to evaluate for this?
Antibody-dependent enhancement. This means that infection with the virus that causes Covid after vaccination could, for some people, result in more serious illness. This occurred in one animal model, for one vaccine against SARS. How is this being evaluated for? What is the sample size needed?
Oh, and for the mRNA vaccines, what adverse events do we even look for? We've never used this type of vaccine in people before.
Lots has been done right with Operation Warp Speed (multiple vaccine types, manufacturing and trials in parallel), but let’s hope they don’t warp the science. There’s no way to stop epidemics without trust. Politicizing data and decisions is essential for trust, and very, very dangerous.
The pandemic ain’t over until it’s over, and it’s nowhere near over. Even with a safe, effective, available, and trusted vaccine, it would be months or years before the risk of deadly outbreaks is down to manageable levels. We need continuous improvement in testing, isolation, tracing, and quarantine. The 3W’s make a big difference: Wear a mask, Watch distance, Wash hands. Improving ventilation and spending more time outdoors also help. Smarter limitations on activity can balance jobs and health. We’ll need to make preparations for vaccination, hoping that safe and effective vaccines become available. These including improving the cold chain and engaging communities. It's past time to begin conversations with communities, sharing what we know and don’t know and listening to concerns and perceptions.
Cases in the United States remain at a high level, increasing in much of the country, and we continue to fail to implement an effective, coordinated response.
COVID This Week: Decreasing Cases, Increasing Danger
(Blog initially published in Tom Frieden’s LinkedIn account https://www.linkedin.com/pulse/covid-week-decreasing-cases-increasing-danger-tom-frieden/)
The latest data show that Covid is decreasing from very high levels to high levels in much of the U.S., but don’t be lulled into a false sense of security—danger is still very present. Schools are reopening and outbreaks are inevitable. And although human immunity against the virus now appears possible, FDA and CDC immunity from political interference is much less so.
First, the trends from last week. National test positivity decreased from 6.2 to 5.7%, which confirms that there has been a steady decrease in cases over the past few weeks. Case rates in the Northeast remain relatively low, and these states are now joined by MI, WV, NM, MT, WY, AK which have relatively low rates. The number of tests done decreased in some states, including Florida. Antigen testing—which is much faster than most PCR testing but less reliable—will make the national positivity number harder to track, and there’s a risk that many antigen tests won’t get reported. State and local health departments need to receive 100% reporting of PCR and antigen tests.

To date, the US has seen more than 500,000 cumulative hospitalizations, 6 million diagnosed cases, 180,000 reported deaths, plus at least another 50,000 or so excess deaths above baseline, which are from a combination of undiagnosed Covid and Covid-disrupted care. To put the U.S. situation into perspective, the US Covid death rate just for last week was more than three times the rate in South Korea since January.
The Latinx population in the U.S. as well as many Latin American countries are being very hard hit by the virus. Many are essential workers who have insufficient protection, are more likely to face crowding, have lack of access to care, and have underlying health problems. Peru now has the highest cumulative death rate in the world, and also has many unreported deaths.
There are high hospitalization rates in Native American, Latinx, and Black communities in the U.S., but these numbers are gradually declining. We can only reopen more by staying safer, masking up, and finding and stopping spread with the box-it-in strategy.

Masks matter. At Resolve to Save Lives, we released a toolkit this week sharing evidence, tools, and best practices for policymakers and communities to promote mask-wearing, which I summarized in the Washington Post. Masks are one of the lowest-cost, most effective tools we have to get more of our economy, education, and health care back. Mask up to keep deaths down. Kudos to Philadelphia for measuring and improving use.

These are troubling times, not just because of epidemiological trends but also because of political interference with science. It’s been said that in war, truth is the first casualty. In this war against a virus, truth can be our strongest weapon.
Indefensible framing by the FDA of emergency use authorization (EUA) for convalescent plasma threatens to undermine trust in the agency. Convalescent plasma is a 100-year old treatment that may work, a bit, for some patients. There’s still so much we don’t know. For example: What antibodies should be used? For which patients? When in the course of illness? What dose? For how long? We need more science and less politics.
The CDC also made an indefensible recommendation, dictated by White House/HHS, that asymptomatic contacts of Covid-positive patients don’t need to be tested. That recommendation is not backed by science. We need to test asymptomatic contacts. If these contacts are positive, their contacts can be identified, warned, and quarantined. Not testing asymptomatic contacts allows Covid to spread. Let’s hope the CDC website gets corrected.
There have been far too many preventable casualties from the failed US response to the pandemic already: lives, jobs, education, and more. We cannot let the FDA and CDC become the next casualties of Covid. We must base decisions on science and insist on complete transparency on data and process.

A Dozen Observations About COVID-19 Immunity
(Blog initially published in Tom Frieden’s LinkedIn account : https://www.linkedin.com/pulse/dozen-observations-covid-19-immunity-tom-frieden/)
Immunity is tricky. We think of it like armor – if we’re immune, we’re protected. But it’s much more complicated. Every day, we learn more about immunity to SARS-CoV-2, the virus that causes COVID-19. On balance, what we’ve learned is good news, but there are important caveats and implications.
First, the good news:
1. Recent laboratory studies suggest – but don’t prove – that immunity from infection with SARS may last many years.
2. These same studies suggest that antibodies, which have been a focus of research, may not be the only, or even the most important component of our immune response.
3. Animal studies suggest that infection protects against re-infection, at least in these animals, at least in a laboratory model, at least for a few weeks.
4. A small but interesting study suggests that neutralizing antibodies in people may be protective against re-infection, at least for some time for some people. It’s not enough to bet your life on, but it’s enough to be optimistic about the potential for immunity.
Now, the caveats:
1. We don’t know how long immunity, if it occurs, will last or how complete the protection is. Overconfidence could lead individuals and communities to let their guard down, which could result in more spread and more death. Testing positive for antibodies does NOT mean you’re immune.
2. We don’t know what proportion of people with natural infection will become immune.
3. We don’t know if some people who get vaccinated will develop harmful immune over-reaction.
4. Even if 20% of the US population has been infected, we’re nowhere near herd immunity. Not all infected are necessarily immune, and, more importantly herd immunity likely requires at least 60% infection rates, and in any case isn’t an on-off phenomenon. When more people are immune, infection spreads more slowly. But because spread is uneven, communities remain vulnerable even if a high proportion of the population has been infected. Getting to herd immunity in the US would require hundreds of millions of infections and at least a million more deaths. That’s not a plan, that’s a catastrophe.
And now, the implications:
1. The likelihood that an effective vaccine will be found is increasing. Why? Because Mother Nature usually does better than our best vaccines, and the ceiling of vaccine efficacy is usually protection after natural infection. But vaccination won’t be quick or simple. We have to ensure it’s safe, effective, available, and trusted.
2. We need to be particularly careful about vaccine safety. Developing immunity — either through infection or vaccination — may result in severe illness. This is why some people get so sick with COVID-19, and likely why dexamethasone, a medication that weakens the immune system, helps some severely ill patients. It’s a concern with vaccination, which could potentially harm a small proportion of patients because of immune over-reaction – either from the vaccination itself, or from exposure to the virus after vaccine-induced immunity. This is being studied in the vaccines being developed and will need to be tracked whenever they are given.
3. It’s possible, once vaccination is widely available, that immunity passports – certificates of immunization (or, potentially, of protective immunity from infection) will become a reality. This is already done (not well) for Yellow Fever. If it helps us reclaim our education, jobs, and economy, this could be a good thing – but there are important risks to be considered. (We outlined some controversies: “…perverse incentives, muddled risk communication messages, violations of patient privacy, diversion of resources, fraudulent certificates, and creation and perpetuation of inequalities, among others.”)
4. We can get to a new normal if we improve control today, stay apart, work together, and prepare for vaccination if and when it becomes available. For now, we need to continue to wear masks, watch our distance, and wash our hands. Our schools and universities need to be extraordinarily careful. In most of the country, we need to keep our bars closed, indoor dining closed, and avoid closed indoor spaces with lots of people present. There may be light at the end of the tunnel, but immunity is definitely not just around the corner!
There’s still more we DON’T know than what we do know about immunity to the new coronavirus. Humility remains very much in order. Learn, share knowledge, discover, move forward carefully, guided by science and a focus on protecting both lives and livelihoods.
Latest in COVIDView: Just when you thought it couldn’t get worse…
Here’s where we are in the US with Covid now. This is based on CDC’s latest COVIDView report, Covid Exit Strategy and other sources.
Outbreaks in the US have gotten so bad, the folks at Covid Exit Strategy added a “bruised red” to their map, signifying states where the virus is out of control. The bruise is spreading.

In the past week, overall test positivity increased slightly, although positivity in commercial labs decreased slightly. Something odd is going on with the commercial lab data—the number of tests reported is way down and we’ll have to wait until next week to know if these trends are reliable.

Look carefully at the public health lab results. Lines are positivity rates, on the Y axis. Note the yellow—young adults—increasing for more than a month. Older adults (blue and green lines) increased sharply last week. That’s not good. Because there’s a lag in deaths we’ll first see an increase in cases. The deaths follow 2-3 weeks later.

Test positivity trends are revealing, but don’t be fooled by test numbers. I don't know why people are wondering if we will have more than 100,000 infections a day in the US. On Saturday there were at least 200,000, possibly many more than that. We diagnose only a small fraction.
Many tests take more than 2-3 days to come back, which means they are of little value. We should know testing rates for each race/ethnic group and ensure all results come back within 48 hours.
Influenza-like and Covid-like illnesses are continuing to increase in much of the country. This syndromic surveillance is an important early warning system that first sounded the alarm in Arizona in late May…

Death rates have declined to near baseline. Hans Rosling got it right: we have a hard time conceptualizing that a situation can be better, but still very bad. We’ve seen a dramatic increase in the use of Remdesivir and a steady increase in plasma treatment in hospitalized patients with Covid. These are promising though unproven treatments.

Here are the most alarming states, with high rates of Covid and high and rising test positivity: Florida, Texas, Georgia, Louisiana, South Carolina, Alabama, Nevada, and Idaho.
Arizona has stabilized at a high rate. California, Utah, and many other states are seeing intermediate levels of spread; the population of California means large numbers of cases there.
Reassuring so far, but still at risk: Northeast, Wyoming, South Dakota. Hawaii and Alaska have low rates with small increases.
Where does the epidemic go from here? This modeling site has performed better than most, using solely deaths and machine learning. Nationally, Youyang Gu estimates there are 4.8 million people with Covid today—1 of every 78 people.

The same site projects 211,500 deaths in the US by the end of October. Leaving Belgium (which counts deaths differently) aside, that would put the US death rate ahead of France, Sweden, Italy, and Spain and about tied with the UK for worst in the world.

Better care and newer treatment can decrease death rates (maybe: plasma and remdesivir early, steroids for some patients late). Even with a vaccine, the virus is here to stay. We need a comprehensive response that will minimize deaths and get to the new normal soon and as safely as possible.
There’s a lot at stake. The chance for our kids to go back to school and for us to get back to work. The chance for our economy to recover. The chance for us to save tens of thousands of lives.
Stay tuned for news Tuesday about a better way to get a nationwide approach despite lack of national leadership.
It’s not about opening schools or our economy, it’s about opening them and keeping them open. We know what to do: follow the 3 W’s—wear a mask, wash your hands, watch your distance (e.g., close restaurants and bars), and box the virus in with strategic testing, isolation, tracing, quarantine.
Latest in COVIDView: US lagging in control, surging in cases
(Blog initially published on my LinkedIn profile https://www.linkedin.com/pulse/latest-covidview-us-lagging-control-surging-cases-tom-frieden/)
Here’s where we are in the US with Covid now. This is based on CDC’s latest COVIDView report, Covid Exit Strategy and other sources.
It’s clear the US does not have COVID-19 under control. Virus is surging, and our response remains fragmented. Only the Northeast is at all reassuring, and those gains are at risk. Reopening schools and restoring our economy are getting much harder.

Test positivity across the US is up to 9.2%. The South Central region is at 17%! See the interesting trends from commercial labs in this graph below. It shows the first decrease in positivity among young adults in 2 months...and now positivity is increasing in older adults. As predicted, what started in young adults didn’t stay in young adults.
We should be seeing testing rates by race and ethnicity—and all tests results must come back quickly. Tests that take more than 48 hours to come back are of little value.
Influenza-like and Covid-like illness visits to emergency departments are rising in 7 of 10 US regions.
Native American, Black, Latinx and other communities continue to be disproportionately affected. They’re more exposed, have more underlying conditions and undertreated illnesses, and also have less access to care. Community engagement, empowerment, and leadership is crucial for progress.
Covidview deaths are below the epidemic threshold, but how long will that last? Overall US deaths are now rising.

Deaths are rising most in the South, Southwest, and West, offsetting the decline in New England, Mid-Atlantic, and Midwest. And this is before young adults spread to lots of older and vulnerable people. The next one to two months will be worse, unfortunately.
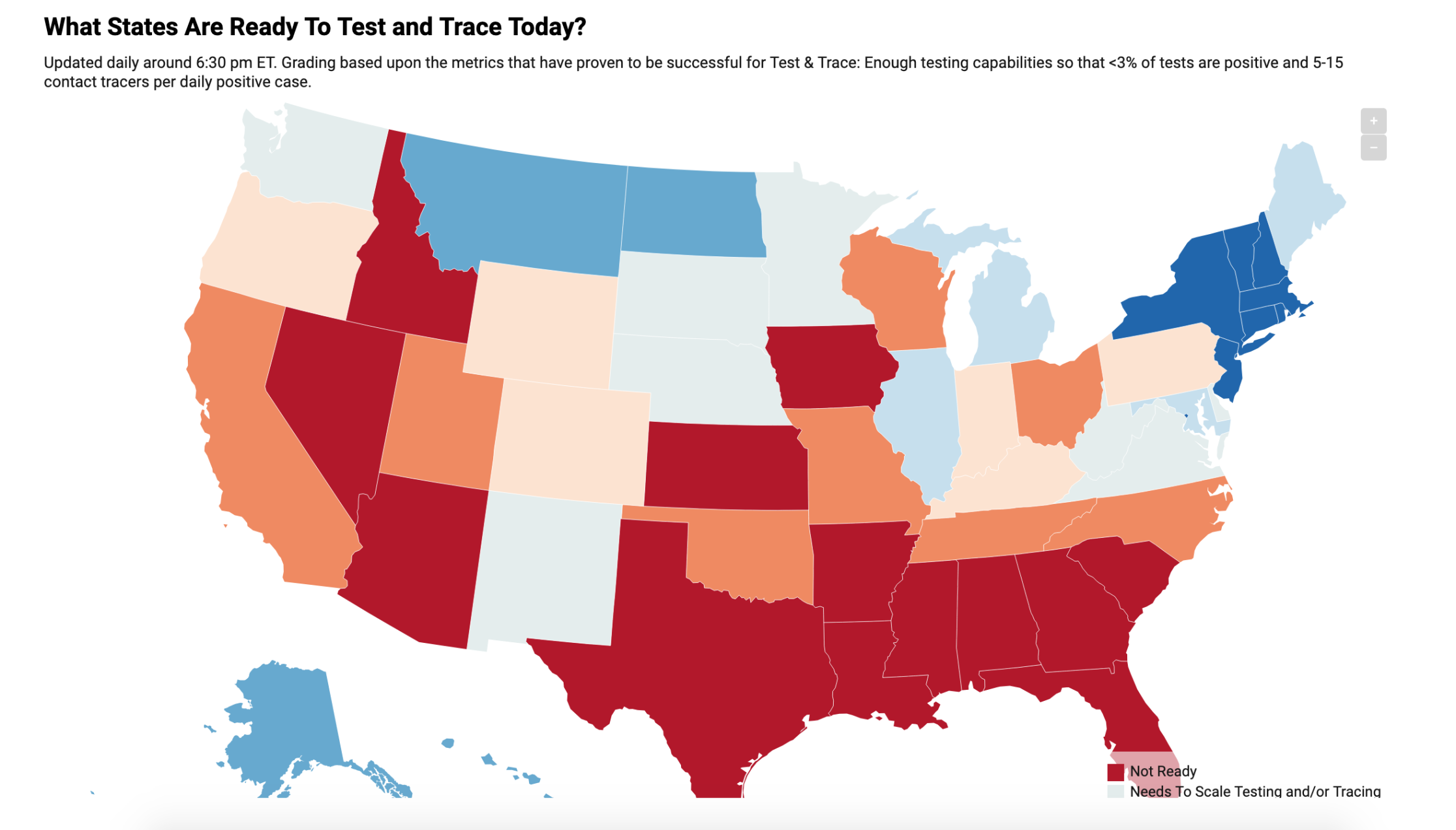
States with the highest Covid burden are least able to test and trace right now.
The situation will get worse before it gets better. Where Covid is spreading and in most of the US it will be essential to close restaurants and bars, stop gatherings of more than a few people, and box the virus in through strategic testing, effective isolation, rapid contact tracing, and supportive quarantine. We all must follow the 3 W’s—wear a mask, wash your hands, watch your distance.
Otherwise, there’s little hope of safely opening schools, no matter what anyone says.
Where are we with the COVID-19 Pandemic? The Good and the Bad as of This Week
(This blog was originally shared on my LinkedIn account: https://www.linkedin.com/pulse/where-we-covid-19-pandemic-good-bad-week-tom-frieden/?trackingId=GnuqPnY5Q26fXQu2W8YIWg%3D%3D)
Another momentous and painful week. With it, another CDC COVID-View report. Below is a quick summary of the key findings.
One big thing to note is what’s not reported: case numbers, which are largely irrelevant. We actually find only about 1 in 10 cases, and the numbers are highly dependent on testing intensity and the testing approaches used.
First, the good news on COVID-10 epidemiology. The percentage of positive tests continues to decrease, as do trends for the proportion of outpatient visits for ILI and CLI (influenza-like illness and COVID-like illness). These proportions can be misleading because when people do not go to healthcare facilities or seek treatment to avoid exposure to COVID-19, the proportions can increase even if infections are decreasing. It’s important to track both the proportion and numbers of ILI/CLI.

Now, two pieces of not-so-good news:
First, in 4 regions, the southeast, southcentral, west coast, and pacific northwest, test positivity has increased.
Second, the positivity rate in kids continued to stay stable or increase.

The leading hypothesis is that adults are bringing infection home to their kids. To remedy this, we should offer housing for the infectious period for all with COVID-19. This is what the best programs around the world are doing. This limits spread and protects families. This should, of course, be voluntary and provide appealing, temporary housing.
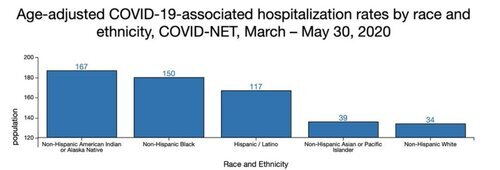
Race/ethnicity inequalities continue to persist, with Native and Black people having 5x hospitalization rates and Hispanic/Latinx people having 4x the hospitalization rates of white people. This disproportionate burden requires a disproportionate response. We must focus on protection, prevention, engagement, and support.
Now, for the most encouraging trend. Deaths continue to plummet. Within a week or two, death rates may be at or near the baseline IF trends continue. Note, the below chart shows the percent of death from pneumonia, influenza, and COVID-19. We use percent, not number, because this is the most reliable indicator.

But, even with this trend, there could still be hundreds of deaths from COVID-19 each day. It’s preventable. It’s tragic. And it represents continued spread and risk of the virus. However, Europe, which is weeks ahead of us epidemiologically, appears to be reopening without rekindling -- yet.
So, we will wait and see. What should you do? What you have been doing. Wear a mask. Wash your hands. Watch your distance from others. Box the virus in: test, isolate, contact trace, and quarantine. Continue to track the pandemic and our response to it. Importantly, protect nursing homes, the homeless, jails, factories, and anywhere where large numbers of people congregate. Hope for the best, plan for the worst.
Down With the Covid-19 Virus, Up With the Economy
Blog initially published on my LinkedIn profile ( https://www.linkedin.com/pulse/down-covid-19-virus-up-economy-tom-frieden/?published=t )
We all want two things: to get back to work and to as normal a life as possible and to not endanger the health of ourselves, our loved ones, and others. Personally, I can’t wait to get back to the gym. The better we control the virus, the sooner we can restart our economy because to protect livelihoods, we must protect lives. And the quicker we get back to work, the healthier we will be.
Last week, Resolve to Save Lives released a four-level, color-coded alert system for COVID-19 that could be implemented by city, state, and national governments — with wide consultation within society.
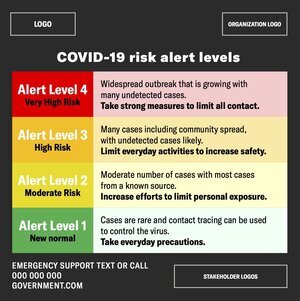
This alert system can achieve three objectives:
It empowers people to protect themselves and their families. There are times when older adults and people with serious health conditions should be extra careful to avoid infection. And businesses, schools, health care facilities, nursing homes, and others need practical information on what they can do at different levels of risk.
It holds government – and all of us – accountable.
It can accelerate progress on reducing risk by focusing on crucially important things we can do to restore economic activity and fight the virus without rekindling the pandemic.
By adopting an alert-level approach, we can empower people, hold governments accountable, and accelerate progress. We can recover our economy without risking our lives.
Groundhog Day in Congress – But This Time it Might Work
This blog was originally published on my LinkedIn profile (https://www.linkedin.com/pulse/groundhog-day-congress-time-might-work-tom-frieden/)
On May 6th, I had the opportunity to testify in front of the House Appropriations subcommittee on Labor, Health and Human Services, Education, and Related Agencies to discuss the COVID-19 pandemic.
As CDC Director, I testified many times in Congress, often with the same message: we have to increase and sustain investment in public health systems in the U.S. and globally to keep ourselves safer. Other than wearing a facemask, using a lot of hand sanitizer, and hearing strong support from many in Congress, there was one major difference this time: it might actually happen.
It was surreal to walk through empty halls of Congress and speak in front of masked representatives, but this reflects our new reality.

Tom Frieden testifying in front of the House Appropriations subcommittee on Labor, Health and Human Services, Education, and Related Agencies
Just projecting from the number of people already infected and being infected now, the virus will have killed at least 100,000 people in the U.S. by the end of the month. But we can get through this. It’s us against them – humans against the virus.
There are 10 plain truths we need to accept in order to move forward productively and effectively.
1) It’s really bad.
In New York City, it’s on the order of the influenza pandemic of 1918-1919.
2) As bad as this has been, we’re just at the beginning.
Until we have an effective vaccine, unless something unexpected happens, our viral enemy will be with us for many months or years. There is no magic bullet. Not travel restrictions. Not staying at home. Not testing. Not Remdesivir. All of those can help, but until and unless we have a safe and effective vaccine, there’s no single weapon that will deliver a knock-out punch.
3) We need to be guided by the data.
We need accurate and real-time monitoring to track trends in symptoms, emergency department visits, tests, cases, hospitalizations, deaths, community mobility, and more. We must work to find cases before they become clusters, clusters before they become outbreaks, and outbreaks before they become explosive epidemics that risk the lives of health care workers and others.
4) We will be able to begin to re-open as soon and safely as possible by basing decisions on data and creating a new normal
Sheltering in place is a blunt but effective weapon: it suppresses spread of the virus but inflicts severe hardship on individuals and the economy. After flattening the curve, the next step is to box the virus in by implementing four essential actions – test, isolate, contact trace, and quarantine. All are crucial; if any one is weak, the virus can escape and spread explosively again. If we do all of these four things well, even if we don’t have a vaccine, we can begin to return our society and economy to a more normal footing.
5) We need to find the balance between restarting our economy and letting the virus run rampant
We’re conditioned to think in dichotomies of A vs. B – but open vs. closed isn’t a true dichotomy. We need to think of this more as a dimmer dial than an on-off switch, with different gradations of open based on what we can do without undue risk. Many measures we’re seeing now – floor markings to denote safe distancing, requirements to use hand sanitizer before entering a building, capacity restrictions in restaurants and stores – may be with us for some time.
6) It’s crucially important to protect the health care workers and other essential staff who are the front-line heroes of this war.
They shouldn’t have to put their lives at risk to care for us.
7) We must protect our most vulnerable people.
Nursing homes and other vulnerable congregate settings house approximately 4 million people in the United States. Unless we take urgent action, at least 100,000 residents of America’s nursing homes will die in the next year, and there could potentially be hundreds of thousands of deaths in all congregate facilities, including among those who work in these locations. We must also act urgently to reduce the higher rates of infection and death among African American, Native American, and Hispanic people.
8) We must invest in a vaccine and therapeutics.
Governments and private companies must join forces to make massive, continued investments in testing and distributing a vaccine as soon as possible, ensuring rapid and equitable access in this country and around the world. Nothing else will enable life to get back to a pre-COVID normalcy.
9) We must heighten, not neglect, our focus on non-COVID health issues in order to increase personal and community resilience.
Underlying conditions greatly increase the risk of severe illness. We need to preserve health care services despite the pandemic. We must take steps to avoid people postponing care for strokes and heart attacks, delaying cancer diagnosis, or deferring essential preventive care because of fear of COVID-19. And there has never been a better time to quit smoking, get your blood pressure under control, make sure that if you have diabetes it’s well-controlled, and get regular physical activity.
10) We can never again be caught so underprepared.
It is inevitable that there will be future outbreaks. What’s not inevitable is that we continue to be so underprepared. The simple truth is that in our increasingly interconnected world, disease spread anywhere is a risk everywhere. If the world is safer, we will be safer here at home.
Future health and economic security can best be protected by changing the way we allocate funds to protect us all from health threats. We have seen the limitations that caps and sequestrations cause for discretionary funding. And we have seen that even mandatory funding doesn’t ensure stable support. We propose a new approach for specific public health programs that are critical to prevent, detect, and respond to health threats. We call this the Health Defense Operations (HDO) budget designation, and it would exempt critical health protection funding from the Budget Control Act spending caps so our public health agencies can protect us.
HDO programs should be required to submit a bypass professional judgment budget to Congress annually. The NIH submits three bypass budgets to Congress every year that explain the true resource needs for cancer, HIV/AIDS, and Alzheimer’s research. Likewise, Congress and the American people must understand exactly what is needed for our public health defense so that Congress can then appropriate the resources required to sustain the public health system we need to keep us safe. This investment can save millions of lives and potentially trillions of dollars. Sustained, baseline funding is the only way we will ensure we are prepared for the next pandemic. Responsible funding means protecting America, and we must also ensure accountability in our spending so that every dollar is used wisely.
Bill Murray is fated to relive the same fate in the classic movie, Groundhog Day. But we can learn from our mistakes. The horror that COVID-19 is spreading around the world can be a wake-up call so that in both the United States and globally we do everything in our power to both tamp down this pandemic and drive down the risk of future epidemics and pandemics. By investing in public health protection, we will honor those lost to this pandemic and protect those at risk from the next.
Dr. Tom Frieden is Senior Fellow for Global Health and the Council on Foreign Relations and President and Chief Executive Officer of Resolve to Save Lives, an initiative of the global health organization Vital Strategies.
10 Areas to be Tracked Both Nationally and in Every State and Community during the COVID-19 Pandemic
During the 2014-2016 Ebola epidemic, the CDC produced a weekly dashboard of the most important interventions, objectively grading each in every affected country as red, yellow or green. For Ebola, interventions were in five domains: command and control, surveillance and epidemiology, case management (including laboratory testing), essential health services, and effective communication.

The dashboard focused attention on interventions most likely to stop the epidemic. With COVID-19, the same five domains are essential. Two additional domains to fight COVID-19 are physical distancing and providing social and economic support. Here’s a starter set of 10 areas to be tracked both nationally and in every state and community:
A well-organized emergency management system with empowered incident managers aligned with political leaders.
Testing available for every patient with pneumonia within four hours, every symptomatic person within 12 hours, and capacity for drive-through testing.
Start contact tracing within hours of case identification; identify contacts for >95 percent of cases, track >95 percent of contacts, test 100 percent of symptomatic contacts, and monitor >95 percent of quarantined contacts for 14 days. This is an enormous undertaking, and both trained people and practical digital tools will be essential. China tracked 700,000 contacts — with fewer cases than the U.S. has.
Provide daily briefings with accurate and timely numbers of those infected, ill and deceased, epidemiologic trends and analysis, along with updated guidance from credible spokespeople.
Protect health care workers with policies, training, and personal protective equipment.
Be sure health care systems can safely surge for large numbers of mildly ill patients, a large increase in patients needing intensive care, and patients needing ongoing, non-coronavirus-related care.
Be able to resume targeted or general physical distancing rapidly if needed.
Support nutrition, learning, mental and physical health and well-being, and social needs during isolation and quarantine.
Engage communities, obtaining information through surveys, assessing adherence to physical distancing recommendations, and using findings of these surveys to improve the effectiveness and reduce the disruption of measures taken.
Coordinate with states and localities so guidance and policies are implemented within 24 hours of publication.
You can read my full piece on this topic in The Hill here: https://thehill.com/opinion/healthcare/489887-well-lose-world-war-c-against-the-coronavirus-if-we-dont-fight-the-right